Anecdotally Speaking
The superfluous, a very necessary thing. --voltaireTuesday, December 26, 2006
Christmas Abscess
It was Friday before the holiday weekend. The staff had been working hard to finish so that the office could close early enough to give everybody a chance to get out for last minute Christmas shopping.
My last patient of the day, my last patient of the week, turned out to be a kind, soft-spoken, elderly gentleman who had been my patient for many years. He waited patiently for me in the exam room.
I picked up his chart and looked at the nurse's notes. It read simply, "infected cyst." He lifted his shirt to reveal a nasty infected sebaceous cyst, fluctuant, tense, pointing, surrounded by cellulitis and painfully tender.
I sighed. I glanced at the clock and then at his chart. He is an insulin requiring Type II diabetic and is ninety-seven years old. Today is his birthday.
"Happy birthday Mr. Grey. How long have you had this?"
"When you get to be my age birthdays don't matter much anymore. I have been hoping it would get better on its own."
Mr. Grey's abscess was incised and drained of its foul putrid puss. The remnants of the sebaceous cyst were cleaned out. The empty cavity was loosely packed with iodoform gauze and an antibiotic and analgesic were prescribed for the cellulitis. Cultures were sent to the lab. Mr. Grey was sent on his way to salvage what was left of his ninety-seventh birthday. Arrangements were made for me to meet him at the office on Saturday to repack the cavity.
So began three brief encounters between four individuals over the coming three-day holiday weekend. My daughter, a third year Vet student, home for Christmas, was my companion and assistant for the dressing changes. Mr. Grey's out-of-town daughter was home for Christmas as well. She served as his chauffer and companion on their trips to the office.
For three days, including Christmas Day, the four of us met at the back door of my office at a predetermined time. I unlocked the door and we went inside to go through our little ritual of the abscess dressing change together.
We four got to know each other a little, to share each other's lives together a little and to just care for each other a little. It wasn't a big deal; it wasn't anything anyone planned. It just happened. It was just something that needed doing.
When Mr. Grey's daughter first met my daughter she asked, "Are you the nurse?" My daughter said, "No, I'm a Vet student." I said, "She's studying to be a doctor. Another doctor in the family." I guess I'm proud about that.
Driving home we had this great discussion about the inflammatory response, wound healing, healing by secondary intention and I'm thinking, "What a great conversation to be having with my daughter."
It was a great Christmas.
My last patient of the day, my last patient of the week, turned out to be a kind, soft-spoken, elderly gentleman who had been my patient for many years. He waited patiently for me in the exam room.
I picked up his chart and looked at the nurse's notes. It read simply, "infected cyst." He lifted his shirt to reveal a nasty infected sebaceous cyst, fluctuant, tense, pointing, surrounded by cellulitis and painfully tender.
I sighed. I glanced at the clock and then at his chart. He is an insulin requiring Type II diabetic and is ninety-seven years old. Today is his birthday.
"Happy birthday Mr. Grey. How long have you had this?"
"When you get to be my age birthdays don't matter much anymore. I have been hoping it would get better on its own."
Mr. Grey's abscess was incised and drained of its foul putrid puss. The remnants of the sebaceous cyst were cleaned out. The empty cavity was loosely packed with iodoform gauze and an antibiotic and analgesic were prescribed for the cellulitis. Cultures were sent to the lab. Mr. Grey was sent on his way to salvage what was left of his ninety-seventh birthday. Arrangements were made for me to meet him at the office on Saturday to repack the cavity.
So began three brief encounters between four individuals over the coming three-day holiday weekend. My daughter, a third year Vet student, home for Christmas, was my companion and assistant for the dressing changes. Mr. Grey's out-of-town daughter was home for Christmas as well. She served as his chauffer and companion on their trips to the office.
For three days, including Christmas Day, the four of us met at the back door of my office at a predetermined time. I unlocked the door and we went inside to go through our little ritual of the abscess dressing change together.
We four got to know each other a little, to share each other's lives together a little and to just care for each other a little. It wasn't a big deal; it wasn't anything anyone planned. It just happened. It was just something that needed doing.
When Mr. Grey's daughter first met my daughter she asked, "Are you the nurse?" My daughter said, "No, I'm a Vet student." I said, "She's studying to be a doctor. Another doctor in the family." I guess I'm proud about that.
Driving home we had this great discussion about the inflammatory response, wound healing, healing by secondary intention and I'm thinking, "What a great conversation to be having with my daughter."
It was a great Christmas.
Sunday, December 24, 2006
Niceness Is Imperative
The relationship between physicians and pharmaceutical representatives is unique. I have worked in an office practice of one type or another for over 21 years in three states and during that time, I have always been called on by representatives of the major pharmaceutical manufacturing companies. I have come to admire and appreciate the general quality and caliber of the type of person that enters this profession. And I acknowledge that the job they have is more difficult than they are allowed to admit and than most people are aware of.
The unique relationship between physicians and pharmaceutical representatives sets us both up I think to exploit the human parts of us that tend to be less noble. Where this kind of thing plays out in obvious ways hardly needs mentioning since it has been discussed extensively. But the more subtle and less obvious influences are more pervasive and exert their effects day in and day out and the brunt of the burden is born by the reps and this is why I think their job is so hard. Let me explain.
The reps are trying to sell their product. They come to the physician as the customer of their product, the one who "buys" the product, the one who must be sold on the product. The physician sees the rep coming to him or her as someone who wants something from them, something of value, something of value that only they can give. They are instinctively defensive, skeptical, expecting to be sold on the product. The physician initially feels no obligation to give anything to the rep. The rep tries to create a desire in the physician to give something, ultimately to "buy" the product.
A crude overview granted, but the way I have seen this play out unfortunately many times is that reps have to be nice to doctors even if they get mistreated because they still have to sell their product to them. And doctors can mistreat reps and the reps will still be gracious and treat them with kindness. Sometimes it can be as small as making them wait more than an hour to talk with them for less than 15 seconds without even looking them in the eye. Or making them wait and then leaving the office forgetting that they are there and not seeing them at all. Or the offenses can be horribly cruel and vicious I am ashamed for my profession to say.
And in defense of the reps, the graciousness and consideration that many of them so munificently give is frequently not insincere, but genuine. A testament to the rich character many of these reps possess, which makes sense. It takes someone with character to accomplish difficult jobs and they have a difficult job.
I am always challenged. When someone treats me nice regardless of how I will treat him or her back, there is no accountability on my part. How I treat them depends solely on my own character. If I return their kindness with unkindness, what does that say about me? However, you could say that I am being manipulated, and that is true. But is trading unkindness for kindness the way to deal with manipulation? I think not.
Kudos reps. You are among the most bright, persistent, kind, interesting, compassionate, talented and tough people I know. And I say that not just because you like me. Because I don't really know if you like me, because even if you did not like me, how would I know?
You are always welcome in my office. And not just because you like me. But it doesn't hurt.
The unique relationship between physicians and pharmaceutical representatives sets us both up I think to exploit the human parts of us that tend to be less noble. Where this kind of thing plays out in obvious ways hardly needs mentioning since it has been discussed extensively. But the more subtle and less obvious influences are more pervasive and exert their effects day in and day out and the brunt of the burden is born by the reps and this is why I think their job is so hard. Let me explain.
The reps are trying to sell their product. They come to the physician as the customer of their product, the one who "buys" the product, the one who must be sold on the product. The physician sees the rep coming to him or her as someone who wants something from them, something of value, something of value that only they can give. They are instinctively defensive, skeptical, expecting to be sold on the product. The physician initially feels no obligation to give anything to the rep. The rep tries to create a desire in the physician to give something, ultimately to "buy" the product.
A crude overview granted, but the way I have seen this play out unfortunately many times is that reps have to be nice to doctors even if they get mistreated because they still have to sell their product to them. And doctors can mistreat reps and the reps will still be gracious and treat them with kindness. Sometimes it can be as small as making them wait more than an hour to talk with them for less than 15 seconds without even looking them in the eye. Or making them wait and then leaving the office forgetting that they are there and not seeing them at all. Or the offenses can be horribly cruel and vicious I am ashamed for my profession to say.
And in defense of the reps, the graciousness and consideration that many of them so munificently give is frequently not insincere, but genuine. A testament to the rich character many of these reps possess, which makes sense. It takes someone with character to accomplish difficult jobs and they have a difficult job.
I am always challenged. When someone treats me nice regardless of how I will treat him or her back, there is no accountability on my part. How I treat them depends solely on my own character. If I return their kindness with unkindness, what does that say about me? However, you could say that I am being manipulated, and that is true. But is trading unkindness for kindness the way to deal with manipulation? I think not.
Kudos reps. You are among the most bright, persistent, kind, interesting, compassionate, talented and tough people I know. And I say that not just because you like me. Because I don't really know if you like me, because even if you did not like me, how would I know?
You are always welcome in my office. And not just because you like me. But it doesn't hurt.
Saturday, December 23, 2006
Living Life On Life's Own Terms
I was driving home one day when I spied black smoke crawling into the cold sky near where I live. It was a thick, heavy, dark smoke with an ominous and dangerous look to it. It curled in a way that looked as if the fire had just started. I was not very far away, so I turned down a nearby gravel road and went to investigate.
As I drew closer, the smoke became thicker, blacker, angrier, until I drove over a rise and could see that that the smoke emanated from a conflagration that completely engulfed an automobile angled into the ditch.
I pulled over and got out to see if I could help. We were on an isolated gravel road at the crest of a rise. Two vehicles traveling down the middle of the road toward each other apparently had collided head-on at the crest. One of those vehicles was now being completely consumed by flames in the ditch.
I was one of the first to arrive at the scene of the accident. There was a lone driver in the second vehicle, the one not burning. As I moved closer I saw a tall thin young girl, a high school student, standing alone, watching the burning wreck. She was in obvious distress. I went to help.
She had numerous small little cuts on her face, the kind that safety glass from broken automobile windshields make. I realize she must have been in the vehicle. She was crying loudly, nearly hysterical. It was difficult to tell what was wrong with her. I ask her if she is all right. She pointed at the inferno and wailed, "My sister is still in the car!"
Her voice was a mixture of anguish and pleading, disbelief and pain. I peered closely at the burning car for the first time and the fleeting idea of rescue flashed in my mind. My only thought however was, "If her sister is indeed in that car, then she is indeed lost." I have never seen an automobile so utterly devastated.
I did the only thing I could. I wrapped my arms around the tall thin young girl standing alone on the deserted gravel road, lost in the anguish of a witnessed horror almost too terrible to describe. Little comfort, I am afraid, when comfort is hardly enough.
Later, I assisted the volunteer firefighters in extracting the burnt remains of the young girl's sister from the wreckage. The collision had jammed the engine block backwards against her foot. We had a difficult time getting it free. Apparently, so did she. She succumbed to the heat of the flames, stretched out through the open door of her car, held back by her trapped foot. Her sister had to watch her burn to death, utterly and completely helpless, powerless to do anything to help her.
To live life on life's own terms is to somehow find a way to face and bear the devastating consequences loss and grief impose on us. That young girl went on to graduate High School, then Nursing School, and now works as a nurse and is raising her own family. We do not see each other much anymore and we do not talk about that day.
Grief and loss is a part of life, yes, but what I have never been able to understand or figure out, in a way that make sense to me, is how to live life with devastating loss waiting to pounce upon you at any moment, at any time, when you least expect it. You cannot live life as if tragedy is about to strike at any moment. Yet you also cannot live life as if there will never be any tragedy.
I guess what I would like to do as I struggle to live life on life's own terms, is to live in the moment enjoying the blessings of life without dragging along unnecessary baggage of dread to contaminate my joy. To quell the famous "Yea, but" response to, "Isn't this great?
We end up living life as if bad things are not going to happen, even though we know they will. It is because we do not know what bad thing is going to happen and when it will happen. It just seems twisted and hypocritical. It seems wrong.
I guess what I really want is heaven. Living life on life's own terms, for me, is putting in time, waiting for heaven.
As I drew closer, the smoke became thicker, blacker, angrier, until I drove over a rise and could see that that the smoke emanated from a conflagration that completely engulfed an automobile angled into the ditch.
I pulled over and got out to see if I could help. We were on an isolated gravel road at the crest of a rise. Two vehicles traveling down the middle of the road toward each other apparently had collided head-on at the crest. One of those vehicles was now being completely consumed by flames in the ditch.
I was one of the first to arrive at the scene of the accident. There was a lone driver in the second vehicle, the one not burning. As I moved closer I saw a tall thin young girl, a high school student, standing alone, watching the burning wreck. She was in obvious distress. I went to help.
She had numerous small little cuts on her face, the kind that safety glass from broken automobile windshields make. I realize she must have been in the vehicle. She was crying loudly, nearly hysterical. It was difficult to tell what was wrong with her. I ask her if she is all right. She pointed at the inferno and wailed, "My sister is still in the car!"
Her voice was a mixture of anguish and pleading, disbelief and pain. I peered closely at the burning car for the first time and the fleeting idea of rescue flashed in my mind. My only thought however was, "If her sister is indeed in that car, then she is indeed lost." I have never seen an automobile so utterly devastated.
I did the only thing I could. I wrapped my arms around the tall thin young girl standing alone on the deserted gravel road, lost in the anguish of a witnessed horror almost too terrible to describe. Little comfort, I am afraid, when comfort is hardly enough.
Later, I assisted the volunteer firefighters in extracting the burnt remains of the young girl's sister from the wreckage. The collision had jammed the engine block backwards against her foot. We had a difficult time getting it free. Apparently, so did she. She succumbed to the heat of the flames, stretched out through the open door of her car, held back by her trapped foot. Her sister had to watch her burn to death, utterly and completely helpless, powerless to do anything to help her.
To live life on life's own terms is to somehow find a way to face and bear the devastating consequences loss and grief impose on us. That young girl went on to graduate High School, then Nursing School, and now works as a nurse and is raising her own family. We do not see each other much anymore and we do not talk about that day.
Grief and loss is a part of life, yes, but what I have never been able to understand or figure out, in a way that make sense to me, is how to live life with devastating loss waiting to pounce upon you at any moment, at any time, when you least expect it. You cannot live life as if tragedy is about to strike at any moment. Yet you also cannot live life as if there will never be any tragedy.
I guess what I would like to do as I struggle to live life on life's own terms, is to live in the moment enjoying the blessings of life without dragging along unnecessary baggage of dread to contaminate my joy. To quell the famous "Yea, but" response to, "Isn't this great?
We end up living life as if bad things are not going to happen, even though we know they will. It is because we do not know what bad thing is going to happen and when it will happen. It just seems twisted and hypocritical. It seems wrong.
I guess what I really want is heaven. Living life on life's own terms, for me, is putting in time, waiting for heaven.
$20 For Your Opinion
We call unsolicited promotional material in our mailbox junk mail and in our email spam. What do we call this stuff when it gets to us by fax machine? These "junk" faxes come to my office all the time and are constantly cluttering up my in-box mixed up with my regular paperwork. As soon as I see that it is junk, I toss it.
However, I wanted to share one with you. It starts out at the top in big letters "$20 For Your Opinion."
Dear Dr. David;
Please follow the link below to participate in our partner's short survey.
In return for your valuable time, they will provide you with aSTART NOW, HERE'S HOW: - Blah, blah, blah...
The reason why I wanted to pause and think about this one for a second is that I was having a conversation with my son about how much money I make. He made the comment that I make a lot of money, which is true. That has not always been the case. Both my wife and I come from families that struggled to make ends meet, and in the early years of our family life, we had our own epochal moments of financial struggle.
Indeed, however, we now are very blessed financially. My son is entering that time in his life when he is getting a perspective on what impact income has on a person's life, lifestyle, their choices and ultimately their future. He is weighing his options and measuring his values, as well he should.
My conversation with him got me thinking when I saw this enticement "$20 For Your Opinion." I remembered a survey I read many years ago where patients were asked what they thought the income was of their own doctor. Invariably, across the board, the patients underestimated the actual income of their doctors. The reasons for this are fascinating and could be the topic another time, but the question in my mind was, "Is $20 a good price for my opinion or not?"
My first reaction would be that the value of my opinion for a "short survey" must be $20 because they say it is. It is in print, in big bold letters at the top of the page, where everyone can see it and read it. It is authoritative, therefore, it must be true, my opinion for a short survey must be worth $20.
However, I have been around for a while and I am a skeptic. Besides, I do not need $20 that bad, so I am going to do some figuring, just for laughs and giggles.
I have a good idea what my opinion is really worth on the open market. It is what I do. I sell my opinion. My value derives from an accumulation of knowledge, experience and skills, which I apply with a measure of sound judgment.
So, I took the survey and determined that to earn the $20 Gift Certificate from Amazon.com it required ten minutes of my time. This promotional company is offering me a $20 Gift Certificate for ten minutes of my time. Ten minutes for $20 dollars. OK, got it.
That is a lot, is it not? I mean, that works out to $120 an hour. $120 an hour is a lot. How many jobs are there where a person makes $120 an hour? Especially jobs that are that easy? Sitting on your butt, clicking on buttons on an Internet computer screen for $120 an hour. Wow, who would complain, sign me up.
Except for one, little, tiny, itty-bitty, teeny-weeny, little, problem. We have 1,000 patients coming to our office every month that pay more than three times that much money for ten minutes of a doctor's time. Now, not all of that money goes into the doctor's paycheck, obviously. There are all of the overhead expenses, and all of that stuff. Nevertheless, even after overhead expenses are paid, I make more money for my ten minutes with the patient than $20.
So you say, "Of coarse you should make more for ten minutes seeing a patient, doing doctor stuff is a lot harder and everything. Making $20 for clicking a few boxes in a multiple-choice survey on the Internet is not the same thing, and so it is OK to expect less money, it is just an easier job. What, you don't expect some outrageous dollar amount just for clicking some boxes on a web page, do you!? You rich doctors are all the same!!! Just because you ...blah ...blah ...blah ..."
Yes of coarse clicking a few boxes is a simple job that is hardly worth paying someone to do. That is not the issue. The issue is what is the value of the time of the person that you are asking to give you time. As I said, I know what my time is worth on the open market. One thousand people remind me what it is every month. If you want to purchase my time for an activity that is important to you, at what rate would I be willing to sell you my time? At one third of my going rate? I think not.
Then who would do this kind of survey you ask? Good question! Now we come to my point. I think that there are two reasons this kind of thing exists. The first is the physician whose income is not exposed to the forces of the market. Let me give you two examples of this kind of physician.
The first example would be a doctor who was not seeing very many patients. In order for the amount of money you earn per patient encounter to impact the amount you earn per hour worked, you have to be busy and have a close to full-time practice. The less busy you are, the less you make per hour, the more attractive a low payment for your time will appear. The second example would be a doctor paid by salary or on a guaranteed income. Then any time spent gaining any extra income would be seen as a bonus, not as time taking away from a more profitably spent activity.
The second reason this kind of thing exists I think is more sinister. It is a scam, a fraud, a swindle, a rip off and a con. There are plenty of doctors out there that do not know what their time is actually worth. When they see "$20 For Your Opinion," they think either that their opinion is actually only worth $20, or there is an appeal to a part of them that actually feels guilty for making a lot of money. Yes, it seems ironic, I know, but if a doctor grew up in a poor family, as I did, then being offered $120 an hour for easy work might seem to them like stealing. It would not cross their mind that they were the one being ripped off by being offered only 1/3 of their going rate. This same type of doctor tends to undercharge patients too, and has a hard time making a go at it in private practice.
Do you know what the worst part of this is? This is why I know it really is a scam in sheep's clothing. This is what is at the end of the short survey:
"In order to send your voucher, we need some basic information. Please fill out the fields below, (mandatory fields are marked with an asterisk), and click on the "Submit" button."
Basic information, hah! Right! This is a list selling company. Fill this out, and you will get so many headaches, you will wish you had been paid way more than $20.
Pitch it. There is no easy way to make money. I like to make money the old fashioned way. I earn it. It is more fun that way anyway.
However, I wanted to share one with you. It starts out at the top in big letters "$20 For Your Opinion."
$20 For Your Opinion
Dear Dr. David;
Please follow the link below to participate in our partner's short survey.
In return for your valuable time, they will provide you with a
$20 Amazon.com Gift Certificate.
START NOW, HERE'S HOW: - Blah, blah, blah...
And help shape better services and information for both patients and physicians!
The reason why I wanted to pause and think about this one for a second is that I was having a conversation with my son about how much money I make. He made the comment that I make a lot of money, which is true. That has not always been the case. Both my wife and I come from families that struggled to make ends meet, and in the early years of our family life, we had our own epochal moments of financial struggle.
Indeed, however, we now are very blessed financially. My son is entering that time in his life when he is getting a perspective on what impact income has on a person's life, lifestyle, their choices and ultimately their future. He is weighing his options and measuring his values, as well he should.
My conversation with him got me thinking when I saw this enticement "$20 For Your Opinion." I remembered a survey I read many years ago where patients were asked what they thought the income was of their own doctor. Invariably, across the board, the patients underestimated the actual income of their doctors. The reasons for this are fascinating and could be the topic another time, but the question in my mind was, "Is $20 a good price for my opinion or not?"
My first reaction would be that the value of my opinion for a "short survey" must be $20 because they say it is. It is in print, in big bold letters at the top of the page, where everyone can see it and read it. It is authoritative, therefore, it must be true, my opinion for a short survey must be worth $20.
However, I have been around for a while and I am a skeptic. Besides, I do not need $20 that bad, so I am going to do some figuring, just for laughs and giggles.
I have a good idea what my opinion is really worth on the open market. It is what I do. I sell my opinion. My value derives from an accumulation of knowledge, experience and skills, which I apply with a measure of sound judgment.
So, I took the survey and determined that to earn the $20 Gift Certificate from Amazon.com it required ten minutes of my time. This promotional company is offering me a $20 Gift Certificate for ten minutes of my time. Ten minutes for $20 dollars. OK, got it.
That is a lot, is it not? I mean, that works out to $120 an hour. $120 an hour is a lot. How many jobs are there where a person makes $120 an hour? Especially jobs that are that easy? Sitting on your butt, clicking on buttons on an Internet computer screen for $120 an hour. Wow, who would complain, sign me up.
Except for one, little, tiny, itty-bitty, teeny-weeny, little, problem. We have 1,000 patients coming to our office every month that pay more than three times that much money for ten minutes of a doctor's time. Now, not all of that money goes into the doctor's paycheck, obviously. There are all of the overhead expenses, and all of that stuff. Nevertheless, even after overhead expenses are paid, I make more money for my ten minutes with the patient than $20.
So you say, "Of coarse you should make more for ten minutes seeing a patient, doing doctor stuff is a lot harder and everything. Making $20 for clicking a few boxes in a multiple-choice survey on the Internet is not the same thing, and so it is OK to expect less money, it is just an easier job. What, you don't expect some outrageous dollar amount just for clicking some boxes on a web page, do you!? You rich doctors are all the same!!! Just because you ...blah ...blah ...blah ..."
Yes of coarse clicking a few boxes is a simple job that is hardly worth paying someone to do. That is not the issue. The issue is what is the value of the time of the person that you are asking to give you time. As I said, I know what my time is worth on the open market. One thousand people remind me what it is every month. If you want to purchase my time for an activity that is important to you, at what rate would I be willing to sell you my time? At one third of my going rate? I think not.
Then who would do this kind of survey you ask? Good question! Now we come to my point. I think that there are two reasons this kind of thing exists. The first is the physician whose income is not exposed to the forces of the market. Let me give you two examples of this kind of physician.
The first example would be a doctor who was not seeing very many patients. In order for the amount of money you earn per patient encounter to impact the amount you earn per hour worked, you have to be busy and have a close to full-time practice. The less busy you are, the less you make per hour, the more attractive a low payment for your time will appear. The second example would be a doctor paid by salary or on a guaranteed income. Then any time spent gaining any extra income would be seen as a bonus, not as time taking away from a more profitably spent activity.
The second reason this kind of thing exists I think is more sinister. It is a scam, a fraud, a swindle, a rip off and a con. There are plenty of doctors out there that do not know what their time is actually worth. When they see "$20 For Your Opinion," they think either that their opinion is actually only worth $20, or there is an appeal to a part of them that actually feels guilty for making a lot of money. Yes, it seems ironic, I know, but if a doctor grew up in a poor family, as I did, then being offered $120 an hour for easy work might seem to them like stealing. It would not cross their mind that they were the one being ripped off by being offered only 1/3 of their going rate. This same type of doctor tends to undercharge patients too, and has a hard time making a go at it in private practice.
Do you know what the worst part of this is? This is why I know it really is a scam in sheep's clothing. This is what is at the end of the short survey:
"In order to send your voucher, we need some basic information. Please fill out the fields below, (mandatory fields are marked with an asterisk), and click on the "Submit" button."
Basic information, hah! Right! This is a list selling company. Fill this out, and you will get so many headaches, you will wish you had been paid way more than $20.
Pitch it. There is no easy way to make money. I like to make money the old fashioned way. I earn it. It is more fun that way anyway.
Perfection: The Unspoken Physician Performance Contract
Doctors have to be perfect. Everyone knows it. Patients know it and doctors know it. It is just that no one is allowed to say it in so many words or talk about it in that way. That is because we all know that it is an expectation that is not fair.
Unfair because doctors are human and humans cannot be perfect. Humans make mistakes and so doctors by default must make mistakes too. However, doctors are not allowed to make mistakes. They cannot make mistakes, must not make mistakes. They must be perfect.
Doctors are taught this in their training. If a young doctor makes a mistake, they are instructed to learn from their mistake so that they never make the same mistake again. They progress through their experiences to a place of having all of the mistakes worked out of them, a place where they can practice their perfection.
For the sake of humanity, for the sake of their patients, physicians agree to take on the impossible burden of perfection, at great personal sacrifice, in order to serve those that need them.
The pervasive expectation of perfection in medicine and the striving it engenders has led to phenomenal advances in the capabilities of health care, remarkable achievements.
It is ironic that the more successful medicine becomes in its quest at approaching perfection, the more intense becomes the demand for that perfection, and the more difficult it becomes to actually reach it. Feeding the beast only makes it hungrier, and the food becomes scarcer. It has been said that medicine's success has been its own undoing.
Voltaire warned, "The best is the enemy of the good." Sometimes good enough is just that, good enough. Since perfection is ultimately unattainable, its quest is ultimately fruitless. Seeking perfection tends to freeze us into inaction.
However, it is popular today to look at Voltaire's phrase turned around, as best selling author Stephen Covey, Ph.D. puts it, "The enemy of the 'best' is often the 'good.'" Another way of thinking about this is saying the adequate is the enemy of the excellent. Saying something is good means settling for something less than the best.
Medicine follows this way of thinking. Good doctors do not settle. They always go for the best. Their patients would not have it any other way and they would not have it any other way.
But what about when doctors mess up? Are they being only human or are they bad doctors? Or does that answer depend on how bad they mess up? Or does it depend on how often they mess up? Would it surprise us if we knew how many mistakes doctors really did make? Would we really want to know?
Unfair because doctors are human and humans cannot be perfect. Humans make mistakes and so doctors by default must make mistakes too. However, doctors are not allowed to make mistakes. They cannot make mistakes, must not make mistakes. They must be perfect.
Doctors are taught this in their training. If a young doctor makes a mistake, they are instructed to learn from their mistake so that they never make the same mistake again. They progress through their experiences to a place of having all of the mistakes worked out of them, a place where they can practice their perfection.
For the sake of humanity, for the sake of their patients, physicians agree to take on the impossible burden of perfection, at great personal sacrifice, in order to serve those that need them.
The pervasive expectation of perfection in medicine and the striving it engenders has led to phenomenal advances in the capabilities of health care, remarkable achievements.
It is ironic that the more successful medicine becomes in its quest at approaching perfection, the more intense becomes the demand for that perfection, and the more difficult it becomes to actually reach it. Feeding the beast only makes it hungrier, and the food becomes scarcer. It has been said that medicine's success has been its own undoing.
Voltaire warned, "The best is the enemy of the good." Sometimes good enough is just that, good enough. Since perfection is ultimately unattainable, its quest is ultimately fruitless. Seeking perfection tends to freeze us into inaction.
However, it is popular today to look at Voltaire's phrase turned around, as best selling author Stephen Covey, Ph.D. puts it, "The enemy of the 'best' is often the 'good.'" Another way of thinking about this is saying the adequate is the enemy of the excellent. Saying something is good means settling for something less than the best.
Medicine follows this way of thinking. Good doctors do not settle. They always go for the best. Their patients would not have it any other way and they would not have it any other way.
But what about when doctors mess up? Are they being only human or are they bad doctors? Or does that answer depend on how bad they mess up? Or does it depend on how often they mess up? Would it surprise us if we knew how many mistakes doctors really did make? Would we really want to know?
Thursday, December 21, 2006
Penis Talk
My nurse was making her final notations on the chart before placing it into the chart rack outside of the Exam Room.
"Do you have a name for your penis?" she asked me.
"I beg your pardon," I stammered.
She replied, "I'm taking an informal poll. So far half the girls in the office say that their husbands have a name for their penis."
"Why are you wondering," I asked, not sure that I wanted to know.
"It's your next patient. His penis is named 'Ed'. He said he wanted to talk about 'Ed' and when I asked him who 'Ed' was he said he was having trouble with erections. I never heard of naming your penis before and I was just wondering how often guys give their penis a name. I'm surprised to find out it isn't that unusual."
While I personally have not given my own phallus a moniker to call it's own, I am aware of the practice, although I do not know how common it is. I certainly do not remember anyone calling his penis by name in my office; so, this did seem a bit odd. I approached my next patient with a little trepidation.
After exchanging the customary pleasantries, I asked him the reason for his visit. He calmly stated that he wanted to talk about "Ed."
"My nurse was right," I thought to myself, "this is going to be awkward."
"Ed?" I said aloud, and then trailed off, waiting for him to fill in the expectant silence.
"Yea, you know. Ed."
He pointed at the poster hanging on the wall next to the exam table. In big bold letters it read, "Do You Have Symptoms of E. D.?" The poster went on to encourage patients to bring up the subject of E. D. (Erectile Dysfunction) with their doctors, because new effective treatments are now available.
I took care of my patient and his E. D. problem. Then I could not wait to finish our visit to get out of the room to tell everybody who 'Ed' was. Fortunately, our nurse was very professional and my patient never knew that she thought his penis was named 'Ed'. That day we all learned something about penises and their names, about sexual issues and talking about them in the doctor's office and about E. D. (Erectile Dysfunction) in general and how to better serve our patients.
The E. D. posters have helped to break the ice for many conversations regarding an embarrassing subject. However, no one has since ever said that they wanted to talk about 'Ed'!
"Do you have a name for your penis?" she asked me.
"I beg your pardon," I stammered.
She replied, "I'm taking an informal poll. So far half the girls in the office say that their husbands have a name for their penis."
"Why are you wondering," I asked, not sure that I wanted to know.
"It's your next patient. His penis is named 'Ed'. He said he wanted to talk about 'Ed' and when I asked him who 'Ed' was he said he was having trouble with erections. I never heard of naming your penis before and I was just wondering how often guys give their penis a name. I'm surprised to find out it isn't that unusual."
While I personally have not given my own phallus a moniker to call it's own, I am aware of the practice, although I do not know how common it is. I certainly do not remember anyone calling his penis by name in my office; so, this did seem a bit odd. I approached my next patient with a little trepidation.
After exchanging the customary pleasantries, I asked him the reason for his visit. He calmly stated that he wanted to talk about "Ed."
"My nurse was right," I thought to myself, "this is going to be awkward."
"Ed?" I said aloud, and then trailed off, waiting for him to fill in the expectant silence.
"Yea, you know. Ed."
He pointed at the poster hanging on the wall next to the exam table. In big bold letters it read, "Do You Have Symptoms of E. D.?" The poster went on to encourage patients to bring up the subject of E. D. (Erectile Dysfunction) with their doctors, because new effective treatments are now available.
I took care of my patient and his E. D. problem. Then I could not wait to finish our visit to get out of the room to tell everybody who 'Ed' was. Fortunately, our nurse was very professional and my patient never knew that she thought his penis was named 'Ed'. That day we all learned something about penises and their names, about sexual issues and talking about them in the doctor's office and about E. D. (Erectile Dysfunction) in general and how to better serve our patients.
The E. D. posters have helped to break the ice for many conversations regarding an embarrassing subject. However, no one has since ever said that they wanted to talk about 'Ed'!
Sunday, December 17, 2006
Baby Lester's Desperate Circumstances
 Dr. David and Dr. Cindie sat looking into the open box between them. It contained medical supplies donated by a pharmaceutical company for the upcoming medical mission trip. It was February 2004 and a team of sixteen lay volunteers from a small rural church in South Dakota was going into the jungles of Peru for a one-week mission.
Dr. David and Dr. Cindie sat looking into the open box between them. It contained medical supplies donated by a pharmaceutical company for the upcoming medical mission trip. It was February 2004 and a team of sixteen lay volunteers from a small rural church in South Dakota was going into the jungles of Peru for a one-week mission.This particular box arrived just a few days before they left. After spending months collecting and packing as many supplies as possible, it would be a challenge to find additional space to pack and bring the medications contained within this box. However, there was never a question in the doctor's minds that a way would be found. The pharmaceutical company had generously donated a large amount of a potent, highly effective, injectable antibiotic. Not a has-been product, but a state-of-the-art, front-line product.
The doctors counted the doses and quickly realized this donation was worth thousands of dollars. They were filled with gratitude for those who would give such a precious gift, and for seeing the hand of God blessing the preparations for this trip in such an extraordinary way.
Dr. David and Dr. Cindie had been to the remote jungles of the Amazon River before and they understood the desperate needs of the people they would see. It was breathtaking to imagine what might now be possible. Dr. David posed a prediction: "The medicine in this box is going to save someone's life."
Not long later, it was Thursday of the weeklong mission to Peru, when two team members and Dr. David were making house visits along the jungle river. Dr. David had a portable medical bag with him to look after whatever basic medical needs there might be. These people have no regular access to health care and the needs are very great.
While visiting at one home, a small, motorized canoe pulled up to shore and dropped off a young woman holding a small baby in her arms. The baby's name was Lester. Quickly an urgent call went out. "Get Dr. David, there is a sick baby here."
On approaching the shore and seeing the mother, Dr. David could make out the fear and desperation on her face. With only a glance at the baby in her arms, he recognized that this unfortunate child was not only gravely ill, but he was dying.
Dr. David felt profoundly helpless in that moment. If this dying baby were in a modern American hospital emergency room, he could bring to bear all of his hard-earned medical knowledge and skill along with readily available innovative technology and aggressively save the life of this helpless infant.
Instead, they were standing on the mud bank of a parasite-infested tributary of the Amazon River, deep in the tropical rainforest. To Dr. David, the desperateness and hopelessness of the situation was so tangible that it seemed as if a heavy shroud was pushing him down, as real and as pervasive as the inescapable energy-sapping humidity.
Closer inspection revealed that the infant most likely suffered from pneumonia and was progressing to respiratory failure. The baby was working so hard to cough and to breathe that he could no longer feed. He was becoming dehydrated. The infection was spreading to the bloodstream, what doctors call "sepsis," a vicious medical process that ends in death. Without appropriate and timely medical intervention, there is no hope of recovery.
Dr. David explained that they could do nothing there. They must get back to the medical boat. Baby Lester and his mother were loaded into the speedboat and off they went.
Back at the medical boat, Dr. Cindie and non-medical lay assistants began to treat baby Lester with everything they possibly could. IV fluids, breathing treatments, oxygen. And the precious antibiotic that had been donated. This medicine has the unique property of remaining effective in the blood stream for twenty-four hours after an injection.
When all that could be done was done, Dr. Cindie asked Lester's mother if she was a Christian. She said yes, and Dr. Cindie asked if they could pray. After praying Lester's mother, her anxiety dissipated, exhibited gratitude, and a surprising amount of peace. Exhausted, she was able to lie down and rest, the first time in many days.
When Lester's mother had rested, she asked to take her baby back home with her. She was satisfied with everything done for Lester. Unfortunately, Lester showed no signs of improvement and the medical team wondered if anything they did had improved the baby's prognosis at all. The situation seemed so grave; the baby seemed so far gone.
Before leaving, Dr. Cindie wanted to be sure that the mother was aware of the situation, and did not harbor unrealistic expectations. They did not expect the baby to survive, despite the best medical treatment efforts and despite the belief and faith that God could even if they could not. Not that there was no hope, but to be realistic, to be reasonable in what the situation was they faced.
It was clear his mother understood. In her peace, she would accept whatever the outcome, and in gratitude to the team, for the gift of care she and her baby had received. Arrangements were made to take them back home and visit them again the next day, the last day the team would be in Peru before going back to the United States; a home visit to give the baby another medical treatment. Final prayers were said and then they left. No one knew if they would ever see baby Lester alive again.
The news of what happened with Lester that day had spread around to everyone by Thursday evening. Lester was supported in prayer, and there was much speculation on what the team would find on the next day's home visit. Would Lester survive? Was the gift of the medicine for this trip, for this week, so that Lester's life could be saved? Certainly, it was difficult to imagine anyone needing it more badly than Lester did.
A large team of volunteers formed to travel to Lester's home Friday morning. The speedboat was full. The mood was serious, somber. Chances were good that they would find Lester had not survived the night. However, in this boat, on this morning, there was no despair. No, there was hope, faith and trust in a faithful God that loved them and loved Lester and loved Lester's mother.
The group arrives and quietly, reverently makes its way to the primitive one-room thatched-roof home of Lester and his family. To the relief of all, and with gratitude to God, the weak, sickly cry of baby Lester could be heard as the group approached, a welcome sign that Lester had indeed survived the night. It was difficult to tell if Lester was any better, but to the trained perceptions of the doctors, they thought Lester was showing very subtle signs of improvement, and they were very encouraged.
The room was dark and crowded. Video recorded the event. Mother lovingly cradled her critically ill infant as he held on to life tentatively with every labored gasp of his breathing. Dr. Cindie administered with deft skill her medical treatments, injecting again the powerful lifesaving medicine that had been donated so generously for this very purpose.
The team members crowded around in love and support, an expression of powerful empathy, a spontaneous caress here, an embrace there. There was a powerful sense by all who were there, of an unspoken longing for wholeness and healing, understood by God as a non-verbal prayer of profound faith, a resonation with God's will.
Bill Lake, in the finest tradition of lay ministry, a large equipment mechanic by trade, after spending the week on this mission pounding countless nails to construct a church building, in the most gentle way possible laid his hand on Lester's head, and led the group in prayer.
Goodbyes were said and the team returned to the United States. The video of Lester was shown to thousands of people. However, this was a story without an ending. Did Lester recover? Did he survive? If he did, that would sure make a good ending to the story. Nevertheless, chances are that he did not survive, but that he died. Many were convinced God's purposes were served no matter how it turned out ultimately. However, there was an ongoing sense of loss, of incompleteness, in not knowing how things turned out.
Reflecting on these events and watching the video of Lester brought many who were there to believe that the most important thing that happened to Lester on that trip was prayer. The touch, faith, courage and obedience of Bill Lake somehow reached the very heart of God. No one who was there can watch the video, no matter how many times they have seen it, and not sense again the power of God in that electrifying moment.
The story now has an ending. It came a year latter when another team returned to the same river. Would it be possible to find Lester's house one year latter? Would his family still be there? Would anyone be able to tell us what happened?
Drs. David and Cindie were on this trip as well as Bill Lake. As they passed up and down the river, they could not be sure which house it was. Moreover, time constraints limited how much time they could search. Dr. David, for one, was not sure he wanted to know, thinking that holding on to the hope that Lester might have survived would be better than finding out that he did not. Bill however, was confident. "I can't tell you how I know," he said, "but I know baby Lester is alive."
On the last trip down this river, they passed a house they thought might be Lester's house, and a woman washing cloths in the river that might be Lester's mother. They could not be sure. They nearly kept going without stopping. However, they had them turn around the boat and go back to check. "We can't come this far and miss our chance to find out," they reasoned.
Tentatively, with trepidation, they pulled in close. The woman certainly did look like Lester's mother. The question was very simple and very direct. "Does a baby named Lester live here?" Then the answer, "Yes, he is in the house taking a nap." There was an instant flood of great joy. The second question, "Do you remember us from one year ago when Lester was sick?" "Oh, yes," Lester's mother beamed. There were embraces and an invitation to the house.
The anticipation of seeing Lester, now a healthy one-year-old toddler, intensified as they moved into the house. He was asleep in a hammock. He was absolutely, perfectly beautiful. He was truly a gift from God, full of unlimited potential. Pictures were quietly taken trying not to disturb his slumber. Nevertheless, the flashing lights caused him to stir. He roused, and blinking his sleepy eyes, he tried to take in the startling sight of his usually peaceful house filled with pale white strangers. He almost looked like he would cry, but his mother held him close, comforting him.
Everyone made their acquaintance with Lester; there were more pictures, gifts, candy, prayer and good byes. His mother related that baby Lester battled many months after we left before finally overcoming the illness that nearly took his life. Now he was perfectly fine, healthy in every way.
Why did Lester survive? Because a group of Americans used their vacation time to travel to this remote place in order to help? Because a pharmaceutical company donated life saving medicines that the team could take with them and use? Because Lester's mother brought him to the exact place he needed to be to get the help he needed? Because ultimately trust was placed in God through prayer? Perhaps one or all of these reasons, or perhaps none of them. What is certain though, in the minds and hearts of those touched by Lester, that they have seen the hand of God at work.
Swimming with Piranha
 I am going to Peru again. I am taking a group of people from the cornfields of Iowa into the jungles of the Amazon. This will be the fifth group I have taken into one of the most remote and exotic places on earth. We are buying tickets and getting passports. Soon we will be getting vaccines and planning what to bring. From start to finish, this venture is exhilarating, rewarding and fun.
I am going to Peru again. I am taking a group of people from the cornfields of Iowa into the jungles of the Amazon. This will be the fifth group I have taken into one of the most remote and exotic places on earth. We are buying tickets and getting passports. Soon we will be getting vaccines and planning what to bring. From start to finish, this venture is exhilarating, rewarding and fun.My first trip into the jungles of South America was not leading a team of excited Cornhusker and Hawkeye volunteers however. It was just my High School son and I, joining a group going into the Orinoco River Delta of Venezuela. We were looking for adventure. I was looking for a way to capture my son's attention at a time in his life when it is difficult to attract a young man's attention.
The experiences of that week profoundly affected my life, as it did my son's. He recently wrote an essay about his experiences in the jungle of Venezuela and I found his recollections and insights remarkable and poignant. He has challenged me to recount and record everything I can remember of that weeklong trip. When in your life has a single week mattered so much that you would want to record every detail that you can remember of it? My son and I shared such a week. How remarkable.
I watched my son dispense life-saving medicine to hundreds of people with compassion and sensitivity and love, to women and children with whom he could not communicate. The goldenness of his humanity shone bright and beautiful. My son is a beautiful man.
We brought back our pictures. We told our stories. We touched hearts and awakened the abundant benevolence and kindness of our neighbors. People wanted to go. I took one team, then another, then more. Now this one coming up. Dozens of people going to the jungles, many going over and over again. Bringing their love, and their medicine and their hope.
At the end of our week in Venezuela, Matt and I had a chance to fish for Piranha. We had some for dinner. It was fun. How often in life, are you going to get to do that? While we were eating the fish for supper Matt pointed out to me that the place where we were fishing for the Piranha was the same place where he had been swimming in the river earlier in the week. They told him he would be all right as long as he was not bleeding from anywhere. Hmm, how about that? An Iowa boy swimming with the piranha.
Thank you Matt. Look what you got started.
Succulent Sushi
The other night Cindie and I went out for a nice Sushi dinner. It was a dinner meeting with a drug company speaker. He led a discussion on hypertension treatment, so we learned something about blood pressure and ate some good fresh fish.
I love Sushi. But unfortunately, I do not eat Sushi as often as I would like. Cindie indulges me as infrequently as she can. When we do go out for Sushi, she usually gets some tempera or occasionally a teriyaki chicken. She has never developed a liking for it for some reason. She does not mind the California rolls though. But then everybody likes California rolls.
Fortunately, my kids are like me, they love Sushi too. In fact, all of us taken together, I would say, are maybe fanatical about Sushi. The kids will give me a call if they are out somewhere eating Sushi to tell me how good it is, and share the experience with me. How cool is that?
Aaah, makes my mouth water just thinking about it...
I love Sushi. But unfortunately, I do not eat Sushi as often as I would like. Cindie indulges me as infrequently as she can. When we do go out for Sushi, she usually gets some tempera or occasionally a teriyaki chicken. She has never developed a liking for it for some reason. She does not mind the California rolls though. But then everybody likes California rolls.
Fortunately, my kids are like me, they love Sushi too. In fact, all of us taken together, I would say, are maybe fanatical about Sushi. The kids will give me a call if they are out somewhere eating Sushi to tell me how good it is, and share the experience with me. How cool is that?
Aaah, makes my mouth water just thinking about it...
Losing Consciousness
A patient passed out in my lab in the office the other day. This happens frequently. A reflex can be triggered in most people in the right circumstances called the vaso-vagal reflex. Pain and fear are common triggers, as are emotional stimuli, and getting blood tests taken in the doctors office, on top of feeling ill, is all it takes in many cases.
The vaso-vagal reflex includes a slowing of the heart rate, a dropping of the blood pressure, a feeling of nausea and lightheadedness. The victim will appear pale, break out in a cold sweat, and if they do not lie down, they will loose consciousness. This would be the famous "swoon" or fainting. The loss of consciousness is very brief as long as the person is allowed to lay flat. Laying flat allows blood to flow to the brain and the episode then resolves.
I happen by the lab as my patient was getting the last tube of blood filled. I cracked a little joke to ease the tension a bit and noticed he was loosing his focus. In fact, he was beginning to get a blank stare. Was the joke that bad? No, this was very definitely a blank stare moving into a rolling of the eyes kind of thing. As I called him by his name, I noticed he did indeed look very pale. When he did not answer me, I was certain he was checking out on us.
For many people their first reaction when this is coming on is to get someone up and move them to a room where they can lie down and recover. The patient says, "Oooo, I feel sick!" Then the nurse says, "Come on then, let's get you up and move you over to this room over here so you can lay down." But what happens then is that the patients tend to pass out while they are standing up instead of while they are sitting down. This is not good because it is hard to catch people when they are crashing to the ground from a standing position. Moreover, their heads are then traveling at a higher velocity when they encounter the ground and more damage to the head can occur. We want to avoid this unpleasant outcome.
So, for the sake of the gourd, this is what we do, as undignified as it may seem. "Oooo, I feel sick!" "Come on then, let's have you just slide down off of this chair and lay on the floor for a while." So, that is what we did with my patient. He is a big guy. But with four of us we very carefully and skillfully slide him onto the floor, laid him out, gently placed a pillow under his head, and when he started coming around his first words were, "How did I get down here?"
I am telling this story because I was tickled to death at how this all worked out. You see, we recently moved in to a new clinic that we designed for ourselves from scratch. In the "old" clinic, this patient would now be sprawled out in the middle of the entire lab, which was too small anyway. All operations would have ceased, people would be stepping over him, it was even more embarrassing because he would be out in the middle of everything.
So, I designed the "new" blood draw area with this particular problem in mind. In my minds eye I had imagined how a patient would be handled if they passed out, how we would lay them down, make them comfortable, how we would have plenty of space for what we needed. And it would be relatively discreet. And here it was in real life working out just as I imagined it would. It was great.
The patient recovered fine. He had a glass of water and rested a little while. Then went home. Hopefully that experience will never happen to him again. Next time we need blood from him we will do it with him lying down on a table. No chances.
Just outside the door opening into the blood draw area of the lab are a few chairs for patients to wait their turn to have their blood tests taken. I noticed another one of my patients had been waiting quietly while this passing out thing was going on. When it was all over and it was his turn, I sat down next to him, put my hand on his shoulder and said, "OK, now it's your turn." He looked at me with what I was sure was second thoughts.
The vaso-vagal reflex includes a slowing of the heart rate, a dropping of the blood pressure, a feeling of nausea and lightheadedness. The victim will appear pale, break out in a cold sweat, and if they do not lie down, they will loose consciousness. This would be the famous "swoon" or fainting. The loss of consciousness is very brief as long as the person is allowed to lay flat. Laying flat allows blood to flow to the brain and the episode then resolves.
I happen by the lab as my patient was getting the last tube of blood filled. I cracked a little joke to ease the tension a bit and noticed he was loosing his focus. In fact, he was beginning to get a blank stare. Was the joke that bad? No, this was very definitely a blank stare moving into a rolling of the eyes kind of thing. As I called him by his name, I noticed he did indeed look very pale. When he did not answer me, I was certain he was checking out on us.
For many people their first reaction when this is coming on is to get someone up and move them to a room where they can lie down and recover. The patient says, "Oooo, I feel sick!" Then the nurse says, "Come on then, let's get you up and move you over to this room over here so you can lay down." But what happens then is that the patients tend to pass out while they are standing up instead of while they are sitting down. This is not good because it is hard to catch people when they are crashing to the ground from a standing position. Moreover, their heads are then traveling at a higher velocity when they encounter the ground and more damage to the head can occur. We want to avoid this unpleasant outcome.
So, for the sake of the gourd, this is what we do, as undignified as it may seem. "Oooo, I feel sick!" "Come on then, let's have you just slide down off of this chair and lay on the floor for a while." So, that is what we did with my patient. He is a big guy. But with four of us we very carefully and skillfully slide him onto the floor, laid him out, gently placed a pillow under his head, and when he started coming around his first words were, "How did I get down here?"
I am telling this story because I was tickled to death at how this all worked out. You see, we recently moved in to a new clinic that we designed for ourselves from scratch. In the "old" clinic, this patient would now be sprawled out in the middle of the entire lab, which was too small anyway. All operations would have ceased, people would be stepping over him, it was even more embarrassing because he would be out in the middle of everything.
So, I designed the "new" blood draw area with this particular problem in mind. In my minds eye I had imagined how a patient would be handled if they passed out, how we would lay them down, make them comfortable, how we would have plenty of space for what we needed. And it would be relatively discreet. And here it was in real life working out just as I imagined it would. It was great.
The patient recovered fine. He had a glass of water and rested a little while. Then went home. Hopefully that experience will never happen to him again. Next time we need blood from him we will do it with him lying down on a table. No chances.
Just outside the door opening into the blood draw area of the lab are a few chairs for patients to wait their turn to have their blood tests taken. I noticed another one of my patients had been waiting quietly while this passing out thing was going on. When it was all over and it was his turn, I sat down next to him, put my hand on his shoulder and said, "OK, now it's your turn." He looked at me with what I was sure was second thoughts.
Vanquished Hope
 The limp infant child lay across her lap. His vacant stare and sunken dry eyes revealed that she was losing him. His panting breaths were agonizing as he gave every ounce of life he had left to survive a minute longer. His strength and vigor was nearly gone as weakness visibly weighed on him, pulling him down into a death of stillness and sorrow.
The limp infant child lay across her lap. His vacant stare and sunken dry eyes revealed that she was losing him. His panting breaths were agonizing as he gave every ounce of life he had left to survive a minute longer. His strength and vigor was nearly gone as weakness visibly weighed on him, pulling him down into a death of stillness and sorrow.I looked from him to her, the mother of this dying baby. Oh my heart is pierced! I feel nothing but the sharp pang of fear and pain at the direness of the situation and the helplessness and hopelessness. I am a parent in that brief moment and I feel nothing but what it is like to have my dear child torn away from my arms forever and I feel like I can't bear it.
But I look into her eyes and I could never have been prepared for what I saw. Where I expected a look of expectation and pleading, imploring me to try my best to help however I can, to do what ever I can to save her very ill baby, I saw instead a look of despair more devastating, more penetrating, more consuming than any I could have imagined. And I was beset.
This mother never possessed anything close to an expectation that I could or would make any difference. To her it was of no consequence anything that I said or did that day. As a doctor, of coarse, I did everything that I knew how to do with the equipment and supplies that I had with me to save the life of her baby. We were in the most remote jungles of the Orinoco River Delta in Venezuela. The indigenous people we were seeing had never before been treated by medical doctors, and probably have not been since.
My treatment most likely did not help this little child. And though I am sad to this day about the likely prospect that he died after I left, my greatest grief derives from not being able to impart any comfort to his mother through the act of my kindness. The offering of help motivated by sincere compassion, even if it proves ineffective in the end, usually engenders hope when people face despair, even overwhelming despair.
But not on that day. Not with that mother. Not in that village. And I don't know why. And it bothers me.
I came back home. I continued with my regular routine and busy medical practice. Not a single day has gone by since my encounter with the sick baby and his mother in the jungles of the Orinoco River Delta, when every patient I treat does not come to me with an expectation that I will do what I can to help them.
But I will never forget the day when I looked into the eyes of a young woman who possessed a kind of despair that we know nothing of around here. A rare kind of despair that I don't think any human being should have to bear.
And it haunts me.
Read Between the Lines
 Throughout twenty-one years of private medical practice, my mailbox has been cluttered with an uninterrupted stream of unsolicited enticements to consider opportunities and offers to quit my job, move my practice and relocate to greener pastures.
Throughout twenty-one years of private medical practice, my mailbox has been cluttered with an uninterrupted stream of unsolicited enticements to consider opportunities and offers to quit my job, move my practice and relocate to greener pastures.When I was younger and less experienced, the arrival of such offers occasionally triggered an involuntary interlude of fantasizing on my part. Especially if the advertisement guaranteed salary numbers in a range higher than I currently was making, promised less work, more time off, less stress, better everything and if I had just had a particularly bad week, in my mind, I was packing the bags already.
Oh, and if I offered any encouragement to the places where these things originate from, such as sending for more information, checking a box, returning a reply card, calling a toll-free number, just the slightest hint of interest whatsoever, then the volume of these things in the mailbox triples for about three years before finally dying back down to what seems the background rate of ten or so per week.
I do not even glance at them anymore. They go straight to the trashcan. It has been many years since I had to indulge in one of those greener pasture fantasies, thank goodness. There must be an enormous amount of money spent sending these things out. However, they must work or they would not do it I suppose. They must find doctors for these jobs somewhere by this method.
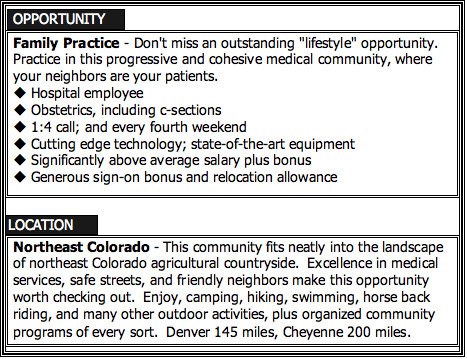
This one caught my eye because it was on a postcard. I thought it would be fun to go through it and read between the lines and translate the hidden meanings and the secret code that I see there as an experienced practitioner. Things may not be apparent to the untrained eye.
"Don't miss an outstanding "lifestyle" opportunity."
This is a good lead off using the lifestyle word. It is a hot-button word in recruiting; it gets people's attention. The docs that are looking for lifestyle practices are interested in the non-monetary rewards; they usually do not want to work that hard. They are docs that are willing to make less money to have more time-off. So, by putting the word lifestyle in quotation marks, what they are really saying is, that this is a nice place to live kind of lifestyle, but you can expect to work your butt off here.
"Practice in this progressive and cohesive medical community..."
Saying this is a "progressive" medical community is a nice way of saying that the docs in this town do not get along. Saying it is "cohesive" means that there is a truce and a pecking order has been established. Guess where the new guy will fit in?
"...where your neighbors are your patients."
This means you are on your own. This place is rural rural remote remote. The nearest consultants and specialists are probably a long way away. Some docs like that kind of excitement, being the Lone Ranger. As long as they know what they are getting into. This also means you are going to work your butt off here.
"Hospital employee"
Most docs take this to mean "we take care of that nasty old business crap you doctors don't like to deal with so you can do what you are really good at which is save lives and take care of sick people" and the docs are happy if they can just practice medicine and collect the paycheck they were promised. However, what it really means is the only ultimate control the docs actually possess is just the ability to leave. That is a position of weakness that many docs do not realize they are in until they find themselves unable to influence matters of significant concern to them.
"Obstetrics, including c-sections"
This means you do not have to compete with specialists to do the things as a family doctor you were trained to do. This would be attractive to many family doctors that are being shut out of medical staffs in urban hospitals because of so called "turf" battles. This also means you are going to work your butt off here.
"1:4 call; and every fourth weekend"
This is "code language"; it represents the most ideal call arrangement for the average family practice. It is an ideal. It never happens in real life. Here is what this is saying, that there are at least three family docs there now. That is all it is saying. Here is a likely scenario. One of the three docs is holding on by his fingernails waiting for you to sign-on so he can finally retire. So, when you get there you end up being on call 1:3 and every third weekend. Except the other two guys get twelve weeks off each year as part of their contract, so half the time you are on call every other night and every other weekend. Until the guy you are sharing call with gets sick while the other guy is on vacation and you are now the only one on call without any breaks and a hundred miles away from any backup and how about that for "lifestyle"?
"Cutting edge technology; state-of-the-art equipment"
What this really means is that they just bought a new heart monitor for the CCU and a new fetal monitor for OB. Never mind that they had to because they could not get parts anymore for the old models. They are very proud of their shiny new expensive machines. They are the first things they show you when they give you a tour of the hospital.
"Significantly above average salary plus bonus"
Ha! I should hope so! Whoever ends up here is going to work their buns off! (I think I have made that point?) The thing is, if the salary was actually significantly above average they would put the actual numbers in the flyer. Not only that, they would set the numbers in the largest type on the page to catch your attention and make sure everybody would notice them. It would be their biggest selling point. No actual numbers means the salary is just average.
"Generous sign-on bonus and relocation allowance"
Ho hum, everyone says that.
"This community fits neatly into the landscape... agricultural countryside."
Again, read rural rural remote remote.
"Denver 145 miles, Cheyenne 200 miles."
What this means, besides rural rural remote remote, is that when you get your chance to leave the other poor bastard to be on call alone by himself, to get away for a medical conference or a vacation, you will have to endure passage on an infamous knee-to-chin, 100 decibel, teeth rattling, vibrating, turboprop, turbulence chasing, regional airline connecting flight, to get to any major airline terminal hub in order to escape to the real world. Moreover, when you get there, sometimes you will wonder if it was worth the trouble. Or, you will give serious thoughts to ever going back. In some places, I bet they never do go back. Which may be why this card came in the mail?
"Enjoy, camping, hiking, swimming, horseback riding, and many other outdoor activities"
What this means is that you will spend many long hours of your life in the hospital ER taking care of people who have injured themselves enjoying camping, hiking, swimming, horseback riding, and many other outdoor activities.
Do I sound jaded and cynical? Maybe. Nevertheless, a word to the wise. Buyers beware.
As for me, I am happy right where I am.
(Want to know what that really means?)
Archives
December 2006 January 2007 February 2007 March 2007 April 2007
![]()
Subscribe to Posts [Atom]